
The Mother of All Black Triangles
"Sometimes a particular case comes along that appears, at first, to be overwhelming. The case described in this article fits that description. However, when this patient emailed my office and inquired about the possibility of flying across the country to have me treat him, I had fortunately done many cases involving hundreds of teeth using the matrix system that I developed to treat dentition afflicted with black triangles, albeit none of this magnitude. I felt absolutely confident that we could achieve a good outcome. The trick was to disassemble the case into bite-sized pieces. This case presents many excellent questions and the additional challenge of severe facial abrasions. I will first review the background of black triangles and of lower incisor complications, and then proceed with the presentation of the clinical procedures used to treat this particular patient."

Treating the Dreaded Black Triangle
This case presents many excellent questions and the additional challenge of severe facial abrasions. First Cosmetic Dentist Dr David Clark reviews the background of black triangle gaps between teeth and of lower incisor complications and then proceed with the presentation of the clinical procedures used to treat this particular patient.
Treating Severely Worn Lower Incisors
Older dental patients present unique challenges that require dentists to turn to innovative treatment solutions. Each patient treatment should be based on a multitude of factors. However, in the end, two simple questions should be posed to every patient who has reached the twilight of their life, defy the odds, and live on, and on, and on. First, do you think that you will live or could live another 5 or 10 years? Second, do want to outlast your teeth or would you like your teeth to outlast you?

The New Science of Strong Teeth
Most restorative dentists - here in Tacoma and elsewhere - have questioned themselves in regards to the way they prepare Class II restorations. I have certainly done so as my 57-carbide mowed through mostly healthy tooth structure, knowing that I was seriously weakening the tooth.
Microscopes for Esthetic Dentistry
One of America’s best-known architects, Frank Lloyd Wright, once said, “The physician can bury his mistakes, but the architect can only advise his clients to plant vines.” Recent dramatic changes in the practice of both restorative and cosmetic dentistry have placed us in a position that is now very similar to Wright’s architect. Dental patients now “grade” their dentists on the aesthetic quality of their results, and the bar goes ever higher.

Patient Centered Outcomes
Renowned cosmetic dentist Dr. David J. Clark, DDS, defines patient-centered outcomes vs process outcomes and promotes a more minimally invasive mindset in the profession that favors preservation and restoration of the natural tooth.

Optimizing Gingival Esthetics
As patients become increasingly aware of the esthetic potential through cosmetic dentistry, there is an increasing demand for smile makeovers with porcelain. In our efforts to create beautiful smiles, we tend to focus on tooth color, shape, proportion and alignment as we are bombarded with restorative choices.

Microscopes & Zero-Defect Dentistry
Initially resisted by endodontists and mainstream dentists, there has been a recent surge of interest in microscope-enhanced dentistry. In endodontics, the microscope is becoming standard equipment. At a recent opinion leader’s forum, the question was posed: “Should microscopes be required for all endodontic treatment?” This incredible swing in endodontic opinion also is being felt in general dentistry.

Is Minimally Invasive Dentistry Better
Just the other day a company car belonging to a local dentist drove by. It was plastered with advertising from the office, heralding the merits of bleaching, lasers, and minimally invasive dentistry (MID). It was at that moment that I realized that it is high time for the profession to quantify, legitimize, and provide research on the noble but troublesome topic of MID. The term minimally invasive has been embraced by the medical community—hospitals and surgeons are now marketing a wide array of MI medical treatments.
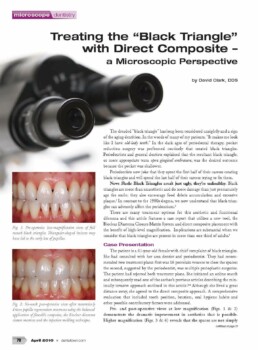
Treating the "Black Triangle" with Direct Composite
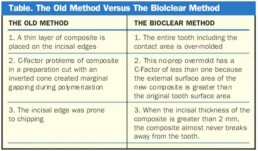
The dreaded “black triangle” has long been considered unsightly and a sign of the aging dentition. In the words of many of my patients, “It makes me look like I have old-lady teeth.” In the dark ages of periodontal therapy, pocket reduction surgery was performed routinely that created black triangles. Periodontists and general dentists explained that the resultant black triangle, or more appropriate term open gingival embrasure, was the desired outcome because the pocket was shallower.
Periodontists now joke that they spent the first half of their careers creating black triangles and will spend the last half of their careers trying to fix them.
News Flash: Black Triangles aren’t just ugly, they’re unhealthy. Black triangles are more than unaesthetic and do more damage than just prematurely age the smile; they also encourage food debris accumulation and excessive plaque.1 In contrast to the 1980s dogma, we now understand that black triangles can adversely affect the peridontium.2
There are many treatment options for this aesthetic and functional dilemma and this article features a case report that utilizes a new tool, the Bioclear Diastema Closure Matrix System and direct composite placement with the benefit of high-level magnification. Implications are substantial when we consider that black triangles are present in more than one third of adults.3
Case Presentation
The patient is a 41-year-old female with chief complaint of black triangles. She had consulted with her area dentist and periodontist. They had recommended two treatment plans: first was 16 porcelain veneers to close the spaces; the second, suggested by the periodontist, was multiple perioplastic surgeries. The patient had rejected both treatment plans. She initiated an online search and subsequently read one of the author’s previous articles describing the minimally invasive approach outlined in this article.1,4 Although she lived a great distance away, she agreed to the direct composite approach. A comprehensive evaluation that included tooth position, bruxism, oral hygiene habits and other possible contributory factors were addressed.
Pre- and post-operative views at low magnification (Figs. 1 & 2) demonstrate the dramatic improvement in aesthetics that is possible. Higher magnification (Figs. 3 & 4) reveals that the spaces are not simply blocked out with composite, but that the papilla has truly been regenerated without the need of surgery.
After a rubber dam was placed, I applied disclosing solution to aid in thorough de-plaquing of the teeth (Fig. 5). Clinicians should be reminded that phosphoric acid placed to etch the tooth will not remove plaque and is a leading cause of discoloration and microleakage of bonded restorations. Other than aggressive spraying of the teeth with a mild abrasive (such as a Prophy Jet or Bioclear Prophy Plus), no mechanical preparation of the tooth is necessary (Fig. 6). A new matrix design specific for diastema closure (Figs. 8-10, Fig. 10 on next page), (Bioclear Matrix System patents pending) allows a smooth, yet aggressive, cervical curvature facilitating direct composite architectures that are extremely conducive to papilla regeneration. This is due to two inherent features. The first feature is the ability to forgo a traditional wedge, and to use the papilla as a wedging force (Use of a traditional wedge creates a flat cervical shape. Flat cervical shapes lack the static pressure needed to regenerate papillae). The second feature is a completely appropriate anatomic shape with exaggerated palatal, interproximal, and facial surfaces. This permits the clinician to simply remove the matrix after photopolymerization with little to no interproximal finishing.
When the finish is extremely smooth and there is a lack of a gingival ledge, tissue health can be ideal, even with a very round embrasure form. This modern view of cervical curvature is in sharp contrast to the outdated notion that prosthetic and restorative embrasures should be flat.
Total etch remains as the most robust method when bonding to large enamel areas, especially on uncut enamel. There is no need to stabilize the Bioclear matrices as they are designed to be self-stabilizing. Alternatively, a metal matrix can be utilized, however it must first be hand burnished and annealed over an alcohol torch (not pictured).
After placing the bonding agent, an initial small increment of flowable composite is carefully injected in both teeth to fill this crucial cervical area (Figure 11). Advanced magnification is of paramount importance for this step. Advanced magnification has become the standard for optimal softtissue response. A flowable composite, rather than a paste composite, is preferred for this first increment. A paste composite would be nearly impossible to place in this “claustrophobic” area without voids and without disturbing the matrices.
Paste composite is then injected into the reservoir of uncured flowable composite. This process is referred to as the “snow plow technique” and the “injection molding technique.”
The concept of injection molded composite dentistry can be compared to impressioning, in which the low viscosity light body material is syringed into subgingival areas, and then followed and partially displaced by a heavier, highviscosity impression material that has appropriate physical characteristics. In this technique, successively higher viscosity materials are applied in sequence, and the bonding resin and flowable composite act as wetting agents, which are subsequently displaced by the heavier paste composite material. A more comprehensive explanation of the injection molding technique will be presented in a future article in Dentaltown Magazine and further information and clinical videos are available at www.bioclearmatrix.com.
The advantage of anatomically shaped matrices is obvious and a welcomed new tool. Once the matrix is removed, the smooth and extremely durable surface is visible (Fig. 12). The new goal of composite dentistry is to do little or preferably no interproximal finishing. That is because a “Mylar-composite finish” has no oxygen-inhibited layer. We have done microscopic evaluation both intra-orally and on extracted teeth and discovered that an undisturbed “Mylar” finish stays mirror smooth for years, and even decades. Conversely, interproximal areas that the dentist “polished” are often gouged, rough, and stained.
How Much Magnification is “Enough” Magnification?
In my previous article, “A Microscope for Every Dentist” (Editor’s note: see p. 42 of the January 2010 issue of Dentaltown Magazine), I described the levels of magnification available for clinical dentistry. A rule of thumb for magnification that addresses the use of composites is listed in Table 2.
Most dentists using microscopes have found that the levels of magnification they use vary greatly throughout a typical day of general dentistry. Placing an occlusal amalgam on a lower first bicuspid is a far cry from evaluating the subgingival disto-bucccal margin during seating of an all ceramic crown on a maxillary second molar. According to the table, I would need 3 x 2 x 2 x 1.5, or 18 power magnification to see well in that example. And frankly I can barely see that margin at 18X in such a case. And the light can’t be too bright. Similarly in the case of black triangle treatment, there are moments such as placement of the flowable when microscopic visualization is invaluable.
Summary
Until now there were very few dedicated tools or techniques for restoratively driven papilla regeneration. Previous attempts at both diastema closure and papilla regeneration using direct composites often ended with significant compromise in periodontal health. The interdental papilla serves as both an aesthetic and functional asset, and anatomically ideal interproximal composite shapes can serve as a predictable scaffold to regain this valuable gingival architecture. The reader is strongly cautioned that to attempt this elective procedure using no magnification and without appropriate materials may not be in the patient’s best interest, and that non treatment or referral is recommended. This extremely rounded, injection molded composite filling technique is new. Once again, technological advancements allow changes to perform techniques that were previously unthinkable. Slowly, the profession will change its thought patterns, retrain its hands and minds, and allow this substantial clinical evolution in restorative dentistry.